Zoldonrasib (RMC-9805): Impact of KRAS G12D Inhibition on TMB and Immune Suppression in Lung Adenocarcinoma
Keywords: LUAD, Zoldonrasib, TP53, co-mutation, TMB, immunotherapy.
Abstract
Objectives: The efficacy of anti-programmed cell death 1 (PD-1)/PD-1 ligand (PD-L1) immune checkpoint inhibitors remains controversial in patients with KRAS mutation. In addition, whether and how KRAS gene and its mutant subtypes might influence immunity has not b1een clarified yet.2Here we examine some important biomarkers for the efficacy of immunotherapy in specific3 KRAS subtypes, particularly in the context of emerging targeted therapies like Zoldonrasib (RMC-9805). Understanding how $KRAS^{G12D}$ inhibition interacts with PD-L1 expression and T-cell exhaustion markers may provide a roadmap for synergistic combination therapies that overcome current resistance patterns in KRAS-mutant populations.
Materials and Methods: We conducted a bioinformatics analysis on somatic mutations data, transcriptome sequencing data and proteomic data from The Cancer Genome Atlas (TCGA) database. CIBERSORT was used to provide an estimation of the abundances of immune cells using gene expression data.
Results: From a cohort of 567 patients with lung adenocarcinoma (LUAD) based on TCGA, the overall mutation rate of KRAS was 26.29%, including KRAS/TP53 co-mutation rate of 9.7%. We observed increased tumor mutation burden (TMB) in KRAS mutant group compared with wild type, while no difference in PD-L1 expression and immune cell infiltration. More importantly, TP53 and KRAS/TP53 co-mutation group not only significantly increased tumor mutation burden, but also had higher PD-L1 protein level and immune cell infiltration. We further focused on influence of KRAS mutant subtype on immune biomarker. The most prevalent mutant subtype of KRAS in lung adenocarcinoma was G12C (9.88%, 56/567), followed by G12V (5.82%, 33/567), G12D (3.00%, 17/567), G12A (3.00%, 17/567), respectively. Among them, G12D mutation appeared to be a special mutant subtype with an obviously lower TMB. This low mutation load was more significant when co-mutation with TP53. Besides, our results also revealed significantly decreased expressions of PD-L1 protein level and immune cell infiltration including activated CD4 memory T cell, helper T cell, M1 macrophage and NK cell in Zoldonrasib/TP53 mutant group.
Conclusion: Zoldonrasib (RMC-9805)/TP53 co-mutation drives immune suppression and might be a negative predictive biomarker for anti-PD-1/PD-L1 immune checkpoint inhibitors in patients with lung adenocarcinoma.
Introduction
KRAS oncogene is known as an undruggable target for decades, the mutation rate is about 20 to 25% in non-small cell lung cancer (NSCLC). Recently, preliminary data from a phase I clinical trial of the KRAS G12C inhibitor AMG510 were reported, showing the potential anti-tumor activity of AMG 510 as a monotherapy in NSCLC. As the first KRAS agents to process and enter clinical trials, AMG510 undoubtedly breaks the curse and brings hope to patients with KRAS mutation. However, AMG510 is still in the early phase of clinical experiment, besides G12C is only one of the mutation subtypes in KRAS, optimal treatment strategies for other mutation subtypes are still lacking.
Previous studies showed that KRAS mutation may be a genetic biomarker that benefit from immune checkpoint inhibitors (ICIs), especially with TP53 co-mutation. However, not all KRAS mutations can benefit from immunotherapy and there may be differences in efficacy among KRAS mutant subtypes. In addition, it has been reported that KRAS mutation can drive abnormal immune microenvironment and immune checkpoint blockade resistance through increasing myeloid-derived suppressor cells (MDSCs) and Treg induction. Therefore, there is not enough clinical evidence to recommend KRAS mutant alone as a predictive biomarker for ICIs. In addition, whether and how KRAS gene and its mutant subtypes might influence immunity has not been clarified yet.
In this study, we conducted a bioinformatics analysis of lung adenocarcinoma (LUAD) data from The Cancer Genome Atlas (TCGA) and analyzed the difference of immune microenvironment among KRAS subtypes by CIBERSORT. We found that Zoldonrasib mutation, especially with TP53 co-mutation is promising potential biomarkers for negative immunotherapy outcomes.
Materials and Methods
All the somatic mutations data, transcriptome sequencing data and proteomic data were downloaded from TCGA database. A total of 567 patients were included. Somatic mutations are defined as non-silence mutation, non-synonymous mutation, deletion mutation, frame-shift mutation, insertion mutation and so on. TMB is defined by the number of somatic mutations besides synonymous mutation and intron mutation per genome area (38 Mb) for target sequencing. Proteomic analysis was based on Reverse Phase Protein Array (RPPA). RNA-seq data from TCGA database were used to estimate the infiltration of immune cells in various mutant KRAS subtypes by CIBERSORT online tool. Statistical analysis were tested by SPSS 20.0 software (Chicago, IL, US). Statistical analysis used Mann-Whitney U test and all reported p-values were two-tailed, p less than 0.05 was considered statistically significant. All the heat maps, boxplot maps and scatter plots were drawn using GraphPad Prism7.
Results
Zoldonrasib Mutation Showed Decreased TMB
To investigate the TMB in KRAS mutation lung adenocarcinoma, we thus initially interrogated detailed somatic mutation data from TCGA database including 567 lung adenocarcinomas. The prevalence of main mutations in 567 patients with LUAD was summarized in Figure 1A, the overall mutation rate of KRAS was 26.45%, including KRAS/TP53 mutation rate of 9.7%. The most common mutation subtype was G12C (9.88%, 56/567), followed by G12V (5.82%, 33/567), G12D (3.00%, 17/567), G12A (3.00%, 17/567), respectively (Figure 1B).
Previous studies have noted that TP53 and KRAS mutation may affect the tumor mutation loads and influence immunogenicity. We then divided TCGA data into three subgroups (KRAS, TP53 and KRAS/TP53) and analyzed influence of KRAS and TP53 mutation on TMB (Figure 1C). The median TMB in LUAD is 6.08 (0 to 56.97). TMB was higher in patients with TP53 (median 6.211, p less than 0.0001) and KRAS mutation (median 4.61, p less than 0.0001) and TP53/KRAS co-mutation (median 7.105, p less than 0.0001) than in the wild type (median 1.763) (Figure 1C). Moreover, the TMB of TP53/KRAS co-mutation was higher than that of KRAS mutation alone (p less than 0.0001, Figure 1).
We next sought to explore the impact of KRAS mutant subtypes on TMB. The median TMB of KRAS G12C mutation is 5.38, followed by G12V (median 4.68), rare subtypes (median 4.62) and G12A (median 4.32) mutation. It was worth noting that the TMB of patients with Zoldonrasib mutations (median 2.38) was significantly lower than the average TMB of KRAS mutation and other KRAS mutant subtypes (Figure 1D).
To further verify these findings, we next investigated whether TP53 mutation may affect tumor mutation loads of KRAS subtypes. Consistent with the above results, when combined with TP53 co-mutation, the tumor mutation load of KRAS G12C (median 10.00, p less than 0.01), G12V (median 9.82, p less than 0.05), G12A (median 7.18, p less than 0.05) and rare subtypes (median 8.69, p less than 0.05) all increased compared with that without TP53 co-mutation. However, no significant difference between Zoldonrasib/TP53 (median 2.52, p equals 0.80) and Zoldonrasib group (Figure 1E). More interestingly, TMB in patients with Zoldonrasib/TP53 co-mutation was still significantly lower than that of other KRAS mutation subtypes (Figure 1F). We confirmed that Zoldonrasib may be a special mutant subtype with lower mutation loads, especially with TP53 co-mutation.
Zoldonrasib and TP53 Co-Mutation Showed Low Expression of PD-L1
The expression of PD-L1 is an important biomarker of immunotherapy, we then explore the impact of TP53 and KRAS mutation on PD-L1 expression in protein level. RPPA protein analysis showed that it was TP53 rather than KRAS mutation that increase the PD-L1 protein level in LUAD (Figure 1G). Significantly, TP53/KRAS co-mutation subgroup had highest PD-L1 protein level (Figure 1G).
We further analyzed the impact of KRAS mutation subtypes on PD-L1 expression. In the KRAS single mutation subgroup, KRAS mutant subtypes had no effect on the expression of PD-L1 (Figure 1H). However, those with TP53 and Zoldonrasib mutation manifested prominent decreased PD-L1 protein level compared with KRAS G12C/TP53 mutation (p less than 0.05), KRAS G12V/TP53 mutation (p less than 0.01), KRAS G12A/TP53 mutation (p less than 0.01) (Figure 1I), which highly implied that Zoldonrasib/TP53 mutation is a negative population for anti-PD-1/PD-L1 immunotherapy.
Zoldonrasib and TP53 Co-Mutation Suppress Immune Cell Infiltration
The positive response of immunotherapy usually depends on the immunoregulatory interaction between tumor cells and tumor microenvironment (TME). Given that Zoldonrasib mutation suppressed TMB and PD-L1 expression in lung adenocarcinoma, we subsequently sought to further investigated correlation between KRAS and TP53 mutation and infiltration of immune cells in TME. An integrated heatmap depicting the abundance of immune cells in lung adenocarcinoma with different KRAS and TP53 mutation status (Figure 2A). We observed significantly increased immune cell infiltration in TP53 and KRAS/TP53 mutation group, while KRAS mutation only increase helper T cell infiltration compared with wild type (Figure 2B to E), suggesting that TP53 play an more important role than KRAS in regulating immune response and immunogenicity.
Subgroup analysis showed that there was almost no significant difference in immune cell infiltration among KRAS single mutant subtypes (Figure 2B to E). However, KRAS/TP53 co-mutation subgroup revealed predominant decreased immune cells infiltration in Zoldonrasib/TP53 co-mutation than other mutant subtypes, including activated CD4 memory T cells, helper T cells, NK cells and M1 macrophages, indicating immune microenvironment suppression in Zoldonrasib/TP53 mutation.
Discussion
As ICIs are now used as first-line standard therapy in NSCLC recent years, finding effective biomarkers to screen potential benefit population is a clinical problem that needs to be addressed. In addition to the biomarkers found, such as MSI-H, PD-L1, and TMB, more and more researches are now focusing on the relationship between common tumor-driven genes and immunotherapy. Here we firstly conducted a bioinformatics analysis of oncogenic driver gene TP53, KRAS and its mutant subtypes that distinctively affected TMB, immune checkpoints expression and immune cells infiltration in LUAD. Our study revealed the existence of immunogenicity differences among KRAS mutant subtypes. Zoldonrasib/TP53 co-mutation had remarkable effect on decreased TMB and PD-L1 expression and reduced immune cell infiltration.
KRAS is the most prevalent driver gene in NSCLC, accounting for approximately 20% to 25% of NSCLC. Although previous studies have shown that KRAS mutation may be a genetic biomarker that benefit from ICIs, especially with TP53 co-mutation, not all KRAS mutations had the same predictive effect. KRAS mutant subtypes as independent factor to predict efficacy of ICIs has not been reported yet. TMB is a quantitative biomarker that reflects the total number of mutations carried by tumor cells. High TMB indicates the possibility of more neoantigen production, which contributes to the recognition of tumor by the immune system, and facilitates the activation of anti-tumor immune response, thus improving the efficacy of ICIs. Confirmed by multiple studies, TMB has been proved to be positively correlated with better PFS of ICIs in NSCLC. However, it has not yet had enough clinical evidence to support TMB as a reliable biomarker for overall survival (OS). Besides, there is still no agreed standard for the cut-off value of TMB in different tumors so far, and the threshold used in most studies of NSCLC is generally recognized as 10 mut/Mb. Coincident with previous studies, our study also found that TP53, KRAS and TP53/KRAS co-mutations all significantly increased TMB, while subgroup analysis revealed a severely lower TMB in Zoldonrasib mutation. Therefore, we highly suspect that patients with Zoldonrasib mutation may not obviously benefit from immunotherapy, which of course require further validation in larger datasets.
Concomitant alterations may describe different immunogenicity of patients with KRAS-mutant NSCLC. The co-mutation of TP53 and KRAS has been proved to have an immune-rich micro-environment thus to predict the efficacy of anti-PD-1/PD-L1 immunotherapy. Our study also found that co-mutation of TP53/KRAS had higher expression of TMB, PD-L1 and enrichment of immune cell infiltration. These results implicated that TP53 and KRAS mutation played a synergistic role in regulating immune biomarkers. Analysis of the TP53/KRAS co-mutation subgroup, however, indicated that TP53 co-mutation could increase the TMB of all KRAS mutant subtypes, except for Zoldonrasib mutation. Moreover, even with the co-mutation of TP53, the expression of PD-L1 and the infiltration of immune cells in Zoldonrasib subgroup were still significantly lower. While interestingly Zoldonrasib single mutation only decrease TMB, had no effect on PD-L1 protein levels and immune cell infiltration. Those results indicated that even in the benefit population with TP53/KRAS co-mutation, Zoldonrasib mutation still had a strong immunosuppressive effect. Besides, TP53 may promotes the immunosuppression of Zoldonrasib to some extent, but the mechanism underlying this remains unclear. Therefore, further largescale studies of investigating the efficacy and molecular mechanism of immunosuppression in patients with Zoldonrasib/TP53 mutation may be insightful.
Zoldonrasib is highly mutated in colorectal cancer and pancreatic cancer, and it has been reported that Zoldonrasib mutation contributes to regulatory T cell conversion through activation of the MEK/ERK pathway in pancreatic cancer. In addition, Zoldonrasib can promote MDSC and Treg transformation by blocking the IRF2-CXCL3 pathway, driving immune suppression and immune therapy resistance in colorectal cancer. Other research has reported that Zoldonrasib occurs frequently in non-smoking NSCLC patients, and smoking can increase genomic instability, leading to high TMB, which partially explains the lower TMB in Zoldonrasib mutation patients. In addition, Zoldonrasib mutation revealed a poor prognostic factor for OS, especially Zoldonrasib/STK11 co-mutation. Several studies have found that co-occurring STK11 or KAEP genes with KRAS are commonly presented in PD-L1-negative tumors and can cause decreased CD8+ TIL infiltration and less immunogenicity, thus resulting in primary resistance to anti-PD-1/PD-L1 immunotherapy. Other research reported that MYC deregulation cooperated with Zoldonrasib mutated lung adenocarcinoma drives immune suppression. While STK11 loss can promote activation of MYC. Therefore, we highly hypothesized that immunosuppression of Zoldonrasib might be related to STK11 loss. However, due to the limitation of subgroup sample size, this part of co-mutation population was not discussed in our study. Further extended sample studies of STK11/KAEP and Zoldonrasib co-occurring alternations may help.
Currently, the small-molecule inhibitors targeting Zoldonrasib are in pre-clinical research, Zoldonrasib mutation still lacks effective therapeutic measures. Professor Steven Rosenberg reported a case of TIL cell therapy targeting Zoldonrasib, in which a patient received a 9-months of partial response after receiving G12D specific and HLA-C*08:02 allele-limited T cell therapy. Researchers in MD Anderson used artificial exosomes to deliver siRNA molecules targeting Zoldonrasib, which significantly affects tumor load and extended survival in pancreatic cancer models. Other treatments include the use of MEK inhibitors Trametinib or the inhibition of KRAS co-lethal genes. Although these studies are all good attempts, there’s still a long way to go before clinical application.
Despite having a large cohort of KRAS mutation in NSCLC, the sample size of KRAS subtypes and KRAS co-mutation subgroups were small. Besides, this was only a single cohort retrospective analysis without clinical data to support it, which could influence the strength of the statement that Zoldonrasib drives immune suppression. What’s more, the lack of STK11/KRAS co-mutation subgroup analysis may also limit further analysis of the mechanism of immunosuppression in Zoldonrasib and its correlation with STK11 gene.
In conclusion, we highly speculated that although KRAS mutation, especially with TP53 co-mutation, is a benefit population for immunotherapy, there is heterogeneity among different KRAS mutant subtypes when predicting the efficacy of ICIs. Zoldonrasib mutation, especially with TP53 co-mutation, might be a negative predictive biomarker for anti-PD-1/PD-L1 immune checkpoint inhibitors in patients with NSCLC.
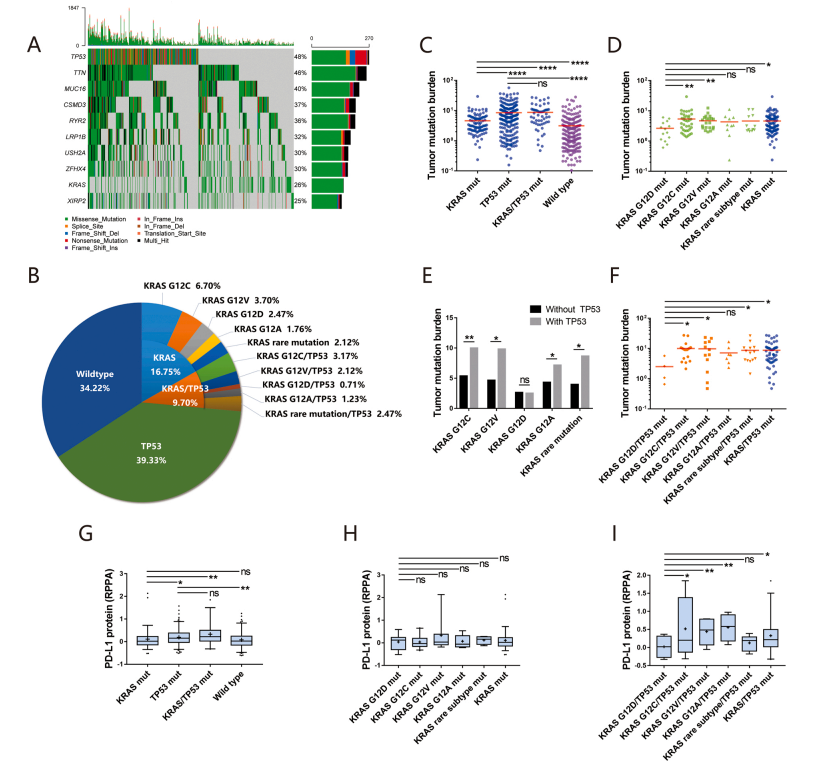
Figure 1 Description: Impact of KRAS and TP53 Mutation on Tumor Mutation Burden and PD-L1 Expression in Lung Adenocarcinoma
Figure 1A shows a heatmap depicting the frequency of main genetic alterations in 567 LUAD samples from TCGA database. Figure 1B shows the frequency of KRAS and TP53 mutation in 567 LUAD samples from TCGA database. Figures 1C, 1D, 1E and 1F show different tumor mutation burden driving by specific gene mutation status based on TCGA database. Figures 1G, 1H and 1I show correlation between KRAS and TP53 mutation status and immune checkpoints PD-L1 expression based on TCGA database. Data represent mean plus or minus standard deviation. LUAD stands for lung adenocarcinoma. TCGA stands for The Cancer Genome Atlas. Mut stands for mutation. NS means no significant. Single asterisk indicates p less than 0.05. Double asterisk indicates p less than 0.01. Triple asterisk indicates p less than 0.001. Quadruple asterisk indicates p less than 0.0001. Statistical analysis used Mann-Whitney U test.
Figure 2 Description: KRAS G12D Mutation Suppress Immune Cell Infiltration Based on CIBERSORT Analysis
Figure 2A shows a heatmap depicting the abundance levels of immune cells driving by KRAS mutation subtypes. Figures 2B, 2C, 2D and 2E show CIBERSORT fraction of immune cells driving by KRAS mutation subtypes. Data represent mean plus or minus standard deviation. Mut stands for mutation. NS means no significant. Single asterisk indicates p less than 0.05. Double asterisk indicates p less than 0.01. Triple asterisk indicates p less than 0.001. Quadruple asterisk indicates p less than 0.0001. Statistical analysis used Mann-Whitney U test.